| Code |
Question |
Answer |
|
AC-29 |
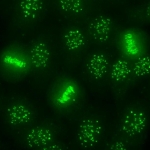
<b>Fine Art with AC-29. </b>Is it critical that all five elements of the subcellular domains associated with the AC-29 pattern be evaluated in order to correctly classify an individual serum as AC-29? In other words, can it be classified as AC-29 with staining of only some of the five elements? |
<p>It is necessary that your microscope settings and your HEp-2 slides be
assessed for the ability to display the AC-29 pattern as described by
ICAP. Some of the elements of the AC-29
patterns may not be readily identifiable. While the staining of the nucleoplasm
and metaphase plate is very evident, the staining of the nucleolar organizer
region (NOR), the nucleolus, and the cytoplasm requires explanation. For the
NOR staining, it is important that different focal levels are analyzed by slowly
adjusting the micrometer knob on the microscope up and down. The cytoplasmic
staining may not be readily visible at lower serum dilutions and may be only apparent
at higher dilutions. The staining of the nucleolus can be more inconsistent and
varies considerably according to the HEp-2 slide brand/lot and other
inter-manufacturer variables.</p><p>Using the reference
standard for anti-Topo I (<a target="_blank" rel="nofollow" href="http://asc.dental.ufl.edu/ReferenceSera.html#text">CAT#: IS2135. ANA #09</a>)
from the Autoantibody Standardization Committee (ASC), one should be able to
identify all five subcellular regions. Otherwise, troubleshooting should consider
adjustments to your microscope settings, the HEp-2 slides and/or reagents used.</p><p>The specificity of the definition of AC-29 pattern for anti-Topo I is
more robust if all five elements are identified. If only the nucleolar staining
is not observed, it is still acceptable to classify the sample as AC-29. The
absence of any of the other four elements is incompatible with the AC-29
pattern provided that the lab can routinely observe the 5 elements using the
ASC or other anti-Topo I internal standards.</p><p>Finally, AC-29 is
likely a problem for automated IFA microscopic systems with a lower numerical aperture
and shallow depth of field because AC-29 pattern recognition requires
examination at different focal planes. </p> |
|
General |
<b>ANA titer reporting. </b>We would also like recommendations on the report of ANA results. For example, when report such as 1:80 dilution AC-1 homogeneous 4+ are made, is it correct to report in crosses (e.g. +++) or only the dilution and the pattern? |
<p>If the indirect immunofluorescence assay
on HEp-2 cells (HEp-2 IFA) is positive at 1/80, it is recommended that the
serum be titered to a dilution of at least 1/640 and thereafter the report
should indicate if the titer is</p><ul><li>>1/80
ûÂã˜ã <1/640<br></li><li>=1/640<br></li><li>>1/640</li></ul><p>A
dilution of 1/640 is suggested as the minimum requirement. Some laboratories do
not dilute beyond 1/640 for logistic and budgetary considerations, while others
who use some automated ANA IFA technologies will obtain digitally calculated
end point titer results.</p><p><u><br></u></p><p><u><b>Additional notes:</b></u></p><p>Although
it may be true that for some antibodies, higher titers are more indicative of
an autoantibody-associated rheumatic diseases (AARD), there are caveats when
considering only the HEp-2 IFA method:</p><ol><li>It is not true for the full spectrum of HEp-2 IFA (ANA) patterns
described by ICAP. The most obvious example is the nuclear dense fine speckled
pattern (AC-2 pattern) that has been shown to occur at high titer in the
general population (1), but uncontrolled experience suggest the same is true for
Golgi, centrosome, and some other cytoplasmic patterns.</li><li>A
point in time ANA is not really that revealing on its own. What is more
important to know is whether titers are decreasing, increasing or staying the
same over time.</li></ol><p><br></p><p><b><u>Reference:</u></b></p><ol><li>Mariz HA, Sato EI, Barbosa SH, Rodrigues SH, Dellavance A, Andrade LE. Pattern on the antinuclear antibody-HEp-2 test is a critical parameter for discriminating antinuclear antibody-positive healthy individuals and patients with autoimmune rheumatic diseases. Arthritis Rheum. 2011;63:191-200.<br></li></ol> |
|
AC-4 |
<p><b>Ro/SS-A and La/SS-B negative in HEp-2
IFA. </b>Can I
get positive Ro and La with negative ANA IFA? How to explain if yes?</p> |
<p>There
may be some significant variations in HEp-2 immunofluorescence assay (IFA) staining
depending on the manufacturer of HEp-2 cell slides employed. Some autoantigens
and epitopes may not be available in some cell preparations. To ensure that the
HEp-2 slide in use can detect anti-Ro60/SS-A and anti-La/SS-B staining,
appropriate reference materials, such as those from <a target="_blank" rel="nofollow" href="http://www.AutoAb.org">www.AutoAb.org</a>, should be used to verify
the HEp-2 slide and other reagents employed in the assay. Experts in the field
also advise to have low titer positive controls to test each new batch of HEp-2
slides for appropriate sensitivity. If well-defined standards for anti-Ro60/SSA
and anti-La/SS-B do not show nuclear staining, this is a clear indication that
the IFA has not been optimized for those autoantigens. The Ro60 autoantigen, in
particular, seems to be labile and can be extracted by mild solvents and even
prolonged exposure to some buffers. </p>
<p> Anti-La/SS-B
- in general, high titer positive <a target="_blank" rel="nofollow" title="Link: null">anti-La/SS-B</a> sera as
determined by solid phase assay (SPA) are expected to be positive in HEp-2 IFA.
It is unlikely that a high titer anti-La/SS-B serum would be negative in HEp-2
cell staining. A caveat is that monospecific anti-La/SS-B sera are very rare
and hence any IFA staining may be related to a second antibody such as anti-Ro60/SS-A.</p>
<p> Anti-Ro60/SS-A -
there are reports that anti-Ro60/SS-A sera positive by SPA may be negative by HEp-2
IFA. Anti-Ro60/SS-A normally gives AC-4 nuclear speckled staining, but in
certain commercially available HEp-2 slides, anti-Ro60/SS-A may be negative. One
manufacturer provides HEp-2 cell slides that overexpress the Ro60/SS-A antigen,
a substrate that reportedly has higher sensitivity and specificity to detect
this antibody than conventional HEp-2 substrates. In contrast, the Ro52 (TRIM21) autoantibody is
not regularly recognized in the HEp-2 IFA test. Thus, a monospecific anti-Ro52/TRIM21
serum may have a completely negative HEp-2 IFA. </p><p></p> |
|
General |
<p><b>Cytoplasmic positive alone is ANA positive or negative?</b> Hello, I would appreciate if you can share with me how to report cytoplasmic staining (without nuclear staining) as ANA positive or negative? <br></p> |
<p>This is an issue that the ICAP committee has discussed extensively but there has been no consensus to date. In many countries, sera showing cytoplasmic staining alone are considered ANA test positive, while in other countries, such sera are considered ANA-negative but cytoplasmic positive. In other jurisdictions, cytoplasmic staining is not reported at all because it is not strictly definable as nuclear staining. There is wide agreement that, sera with cytoplasmic staining alone should not be ignored (1). Other discussions on the topic has suggested renaming he ANA test as anti-cellular antibodies (1), which is consistent with the nomenclature that ICAP has chosen for the various IFA patterns (i.e. AC = anti-cellular). How you report this remains somewhat a local issue. However, whether it is identified as ANA positive or negative has implications for some disease classification criteria. ICAP is working towards a consensus recommendation in the coming year. <br><br>N. Agmon-Levin, J. Damoiseaux, C. Kallenberg, U. Sack, T. Witte, M. Herold, X. Bossuyt, L. Musset, R. Cervera, A. Plaza-ûÂã˜óLopez, C. Dias, Sousa M. Jose, A. Radice, C. Eriksson, O. Hultgren, M. Viander, M. Khamashta, S. Regenass, L. E. Coelho Andrade, A. Wiik, A. Tincani, J. Ronnelid, D. B. Bloch, M. J. Fritzler, E. K. Chan, I. Garcia-de la Torre, K. N. Konstantinov, R. Lahita, M. Wilson, O. Vainio, N. Fabien, R. A. Sinico, P. Meroni, and Y. Shoenfeld. International recommendations for the assessment of autoantibodies to cellular antigens referred to as anti-nuclear antibodies. Ann.Rheum.Dis. 73:17-23, 2014.<br><br></p> |
|
General |
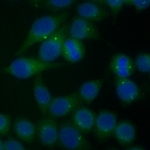
<b>Double IFA protocol.</b> What is the protocol for double IFA that can help to identify, for example, a subcellular compartment such as the nucleolus? |
<p>
Many typical HEp-2 kits come with a fluorescein isothiocyanate (FITC) conjugate such as goat anti-human IgG. For the double immunofluorescence IFA procedure, you need a fluorescence microscope fitted with exciter and barrier filters that are suited to multi-color imaging. In addition, a monoclonal or polyclonal antibody directed against a protein that is specific to the subcellular compartment you are interested in, will be required. This animal antibody will be the tracer for that subcellular domain. If we take the nucleolus as an example, then you need an antibody against a nucleolar protein (e.g. fibrillarin, nucleolar phosphoprotein B23, etc.). Let's say you can obtain a commercially available mouse monoclonal anti-fibrillarin IgG antibody. Most commonly, you will need a red fluorochrome (e.g. rhodamine or Alexa586) conjugated goat anti-mouse IgG to differentiate this from the human anti-nucleolar antibody stained with FITC. It is important that the fluorochrome against mouse IgG is different from FITC and the light signal does not overlap in excitation/emission/barrier filter spectrum used for the FITC conjugate. For the procedure, in the same HEp-2 well, you will incubate the human antibody and the mouse monoclonal anti-fibrillarin antibody. Both should be at a dilution that yield a good fluorescence signal. It is advised that you first optimize the reaction with the monoclonal antibody.
</p>
<p>For the double IFA protocol, there are three options for the primary antibody incubation step:</p>
<p>
1) Human antibody ==> wash (do not allow the well to dry)=> apply the mouse monoclonal ==> wash ==> add a mixture of the two conjugate secondary antibodies at appropriate dilutions ==> wash ==> mounting media (e.g. buffered glycerin) and coverslip
<br>
2) Mouse monoclonal ==> wash ==> apply human antibody ==> wash ==> mix of the two conjugate secondary antibodies at appropriate dilutions ==> wash ==> mounting media and coverslip
<br>
3) Mix of both the mouse monoclonal and human antibody, taking into account that dilution for both is now effectively reduced by one-half ==> wash ==> mix of the two conjugate secondary antibodies at appropriate dilutions ==> wash ==> mounting media and coverslip.
</p>
<p>
In some protocols, it is often helpful to counterstain with DAPI (blue stain). Which of the above 3 options to use may or may not be important. One may work better than the others depending on the specific antibodies you will use. If one method doesn't work well, try the others.
</p>
<p>
You will then be able to see the same field in the microscope under the filters for each of the fluorophores. That will tell you if your human primary antibody stains the same subcellular domain as the monoclonal antibody. It is obviously an advantage to take high resolution photographs of the same field of view and then overlap the images using an image processing program such as Adobe PhotoShop as needed.
</p> |
|
General |
<strong>Nuclear periphery positive and yet center negative?</strong> Some time we observed periphery of the nucleus is stained like positive and center of the nucleus is negative.what is the reason for that ?
|
<p>The nuclear envelope patterns (AC-11 and AC-12) present a distinctive staining of the peripheral border of the nucleus in interphase cells unaccompanied by staining of mitotic cells where the nuclear envelope has broken down. In addition, there may be a faint staining across the interphase nucleus, representing the overlying nuclear envelope. Other than the autoantigen targets represented by AC-11 and AC-12, we are not aware of any other autoantigens that are exclusively located at the periphery of the HEp-2 cell nucleus. Occasionally, some samples yield a nuclear homogeneous staining (AC-1) with a slight enhancement in the vicinity of the nuclear envelope. In our experience, this finding is not consistently observed when we test the sample in other HEp-2 slide brands or with a different lot of the same brand. This observation indicates that this particular fluorescence distribution may be an artifact from cell culture and fixation conditions. One other possibility is the artifact caused by accidental drying of the cell substrate during the incubation steps of the IFA procedure.<br></p> |
|
General |
<div><b>Issue with increasing UV light intensity.</b> I want to clarify when increasing the intensity of UV light, ANA-negative samples may become visible or positive. How to deal with this issue?<br></div><br> |
<p>Increase in UV light intensity can be accomplished with a simple setting change with a modern UV light source and it is clearly important to take note on the effect on ANA positivity in the HEp-2 indirect immunofluorescence assay (HEp-2 IFA). With older microscopes, an increase in intensity often comes with the replacement of new UV bulb. Either increase in light source intensity can affect interpretation of HEp-2 IFA positivity as illustrated in this question. The recommended magnification for HEp-2 IFA is x400 (x40 objective lens) and lower magnification will cause low-intensity positive samples to be interpreted as negative. <br><br>Each laboratory should have a working set of positive and negative human serum sample controls for this specific purpose to ensure that the light source setting is appropriate. A brief discussion on the selection of negative HEp-2 IFA samples is relevant here. HEp-2 IFA cutoff should be determined within the local population using the specific reagents and microscope setting. In a practicing clinical laboratory, it should be clear that there are HEp-2 IFA-negative sera that range from almost completely negative to borderline positive. The latter may be most appropriate to help as reference controls for light intensity setting. Another point to be considered is the fluorescent conjugate. Considering the variability in the microscope settings worldwide it is unrealistic to assume that the ready-to-use conjugate provided with the HEp-2 slide kits will fit all customers. Therefore, it is wise to titrate the conjugate against known negative and low-intensity positive samples in a checkerboard fashion. <br><br></p> |
|
AC- |
I want your impression about my report below
Anti-nuclear and anti-cytoplasmic antibodies ( IF)
Method : IF on HEp-2 cells
Results : ANA :
Pattern :
Titer :
Anti-cytoplasmic antibodies **:
Pattern :
Titer :
*ANA titers more than 1/160 are significant disease indicators . Lower titers of ANA must be interpreted in the context of the clinical information .
** Anti-cytoplasmic antibodies are autoantibodies to cytoplasmic antigens e.g. actin , Jo-1 , mitochondria , ribosomal P ,.. etc
ûÂã ãûÂã ã According to the methods of our lab., more than 95% of SLE patients have ANA titers ûÂã¯ôË 1/640.
Anti-Ro and Anti-La antibodies are recommended for all patients with low and negative ANA results
( if SLE is still suspected ).
Khaled Metwally PhD,
Cairo,Egypt
|
|
|
AC- |
Hola buenas tardes, saludos desde Mûôˋxico.
Tengo una duda y me gustaria saber si pueden resolverla.
He notado que muchas veces el patrûô°n Homogûôˋneo pareciera que esta grumoso y lo doy como DFS-70. Lei en este articulo https://www.jove.com/video/56722/distincin-simultnea-de-monoespecficas-y-patrones-mixtos-dfs70-durante?language=Spanish
y entro en duda si es correcto reportarlo como DFS-70 o como Homogûôˋneo Difuso, Cabe aclarar que el Homogûôˋneo difuso me lo enseûôÝaron en un taller pero como tal no encuentro argumento bibliogrûôÀfico para sustentarlo.
Hello good afternoon, greetings from Mexico.
I have a question and I would like to know if I can solve it.
He noticed that many times the pattern. I read in this article https://www.jove.com/video/56722/distincin-simultnea-de-monoespecficas-y-patrones-mixtos-dfs70-during?language=EspaûôÝol
Digit: DFS-70 or Homogeneous Diffuse, It should be noted that Homogeneous Diffuse taught me in a taller workshop as a bibliographic meeting to support it.
|
|
|
General |
<b>Cutting corners in ANA titer reporting.</b> I want your comment about my way of ANA titration and reporting. Typically I perform only 2 dilutions at 1/40 and 1/160. However, I report titers from negative at 1/40, 1/40, 1/80, 1/160, and further report estimated titers of 1/320, 1/640, 1/1280 and over 1/1280 based on signal intensity. I think I can accurately estimate the titers just from the above 2 dilutions. |
<p>Some laboratories report the fluorescence intensity as numerical (0, 1, 2, 3, 4) or symbols (-, +, ++, +++, ++++) representing a semi-quantitative approximation of the fluorescence intensity. This may be a rough approximation of the actual titer. For economic and practical reasons, many laboratories dilute only up to a given dilution (e.g., 1/640) and report the titer as ûÂã¯ôË1/640 when the sample is still bright at 1/640. In your case, this seems the most appropriate approach rather than ûÂã˜ùguesstimatingûÂã˜ã the end-point titer. This approach is recommended because one cannot really establish a tight correlation between the numerical or symbolic systems and actual titration. For example, some samples look very bright at 1/80, but become negative very early in the titration process whereas some samples that do not show very bright at 1/80 may become even brighter as the sample is titrated to 1/320 and 1/640. This has been referred to as ûÂã˜ùlow dilution antibody systemsûÂã˜ã in the former and ûÂã˜ùhigh dilution systemsûÂã˜ã in the latter. For example, anti-centromere (AC-3) is typically a high dilution system. Also note that one may not be able to discern the true ANA pattern without titering the sample out carefully. In any case, it is not recommended that one states a given titer (e.g., 1/1280) if the real titration process is not performed. Clearly the most scientifically sound approach is to do the actual titrations and report as the titer just below the one at which the reaction becomes negative. <br></p> |
|
AC- |
How can I send a photo of an ANA pattern on HEp-2 for consultation ? |
|
|
AC- |
Do you have a database where I can use it for my research work |
|
|
AC- |
If I have a photo for an ANA Pattern, how can I consult you? |
|
|
AC- |
Dear Sir
We received lot of sample and increase in daily basis.Therefore we need to strength our work capacity and we decide to shift manual method to automation process including sample processing to slide reading.Dear sir, I want to your kind guidelines
to know it suitable for get correct results or any failure in automated machine used. I hope you will help to me about this matter.
Thank you
Regards
wasantha Pushpakumara
|
|
|
AC- |
Dear Sir
We received lot of sample and increase in daily basis.Therefore we need to strength our work capacity and we decide to shift manual method to automation process including sample processing to slide reading.Dear sir, I want to your kind guidelines
to know it suitable for get correct results or any failure in automated machine used. I hope you will help to me about this matter.
Thank you
Regards
wasantha Pushpakumara
|
|
|
AC- |
Dear Sir
We received lot of sample and increase in daily basis.Therefore we need to strength our work capacity and we decide to shift manual method to automation process including sample processing to slide reading.Dear sir, I want to your kind guidelines
to know it suitable for get correct results or any failure in automated machine used. I hope you will help to me about this matter.
Thank you
Regards
wasantha Pushpakumara
|
|
|
AC- |
Dear Sir
We received lot of sample and increase in daily basis.Therefore we need to strength our work capacity and we decide to shift manual method to automation process including sample processing to slide reading.Dear sir, I want to your kind guidelines
to know it suitable for get correct results or any failure in automated machine used. I hope you will help to me about this matter.
Thank you
Regards
wasantha Pushpakumara
|
|
|
AC- |
We have two patients AC-0Negative (Hep2 slide Inova Diagnostic) and DNAds CLIA test positive.ûô¢ It could be possible? We verified the tests again whit the same results. |
|
|
AC- |
Hi Dr Chan,
I hope that the ICAP symposium was very successful. I feel sorry that I could not attend this symposium and the workshop.
Knowing that there is a new classification criteria for SLE with an entry criterion of ANA titer of 1/80 or more do you agree with me that it is not valuable to report the ANA by the intensity of the fluorescence e.g. +, ++, +++ and so on.
What is the recommended starting dilution of ANA for children ?
Khaled Metwally PhD
Cairo, Egypt
|
|
|
AC- |
I had labs drawn a few days ago, my ana screen was positive, my ana titer was 1:80 (H) & the ana pattern was mitotic, spindle fiber AC-25. My dr didnt know what that was, can you help?
Thank you!
Maria Hasalm |
|
|
AC-2 |
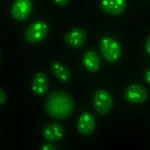
<b>The pseudo-DFS pattern?</b> Some samples yield a nuclear speckled pattern with similar staining at the mitotic chromatin (metaphase and anaphase), very similar to AC-2 (nuclear dense fine speckled pattern), but do not yield a positive result in immunoassays specific for anti-DFS70 antibodies. How should I report such pattern since it is not exactly the AC-2 pattern and there is no anti-DFS70 reactivity? Is this pattern defined by ICAP? |
<p>This is an interesting question and reflects a challenge frequently encountered by ANA laboratories. At the present time, the ûÂã˜épseudo-DFSûÂã˜ô nomenclature has not been endorsed by ICAP or included in the ICAP algorithm. Nevertheless, there is published evidence that not all sera having a nuclear ûÂã˜édenseûÂã˜ô fine speckled pattern with similarly stained mitotic chromatin contain detectable anti-DFS70 autoantibodies. This situation may reflect a HEp-2 IFA pattern that is distinct from the anti-DFS70 positive AC-2 pattern even though it stains the interphase nuclei and mitotic chromatin with a speckled texture. However, the speckled texture is slightly different from the genuine AC-2 pattern (1, 2). The anti-DFS70-positive AC-2 pattern has a speckled texture that is heterogeneous within each nucleus, with some denser speckled areas adjacent to sparser areas; and areas with larger and brighter speckles intercalated with areas with smaller and dimer speckles. The same applies to the staining of mitotic chromatin. Some investigators have suggested the term ûÂã˜épseudo-DFSûÂã˜ô to designate sera that do not have these precise AC-2 staining characteristics (1, 2), The Autoantibody Standardizing Committee offers free of charge reference sera with several HEp-2 IFA patterns and antibody specificities (<a href="http://www.autoab.org/">http://www.autoab.org/</a>), including a reference material for AC-2 pattern (with reactivity to DFS70) (3). This can help in the exact recognition of the AC-2 pattern. Note that the specific autoantibody target(s) and the clinical relevance for the pseudo-DFS pattern but anti-DFS70 negative remains to be published.<br><br>1. Mahler M, Andrade LE, Casiano CA, Malyavantham K, Fritzler MJ. Anti-DFS70 antibodies: an update on our current understanding and their clinical usefulness. Expert Rev Clin Immunol. 2019;15:241-250.<br>2. Infantino M, Bizzaro N, Grossi V, Manfredi M. The long-awaited 'pseudo-DFS pattern'. Expert Rev Clin Immunol. 2019 15(5):445.<br>3. Dellavance A, Baldo DC, Zheng B, Mora RA, Fritzler MJ, Hiepe F, Ronnelid J, Satoh M, Garcia-De La Torre I, Wener MH, Chan EKL, Andrade LEC. Establishment of an international autoantibody reference standard for human anti-DFS70 antibodies: proof-of-concept study for a novel Megapool strategy by pooling individual specific sera. Clin Chem Lab Med. 2019;57:1754-63.<br>û₤ô£ô¢<br></p> |
|
AC- |
Pode haver resultados positivos para dsDNA (ELISA) e nas cûôˋlulas Hep-2 por IFI as mitoses serem negativas?
Como avaliar este resultado?
|
|
|
AC- |
Pode haver resultados positivos para dsDNA (ELISA) e nas cûôˋlulas Hep-2 por IFI as mitoses serem negativas?
Como avaliar este resultado?
|
|
|
AC- |
Hola, habitualmente utilizamos las improntas HEp-2 de BIO-RAD, en algunos pacientes, solemos observar un patrûô°n granular con metafases positivas, muy similar al AC-2 (nuclear granular fino denso) pero que no corresponde a DFS70, ya que lo evaluamos por IFI con cûôˋlulas tranfectadas y nos da negativo para este antûôÙgeno. Este patrûô°n lo observamos especialmente en pacientes con artritis reumatoidea. Mi consulta es, cûô°mo debo informar ese patrûô°n? ya que no corresponde al AC-2 ni a ningûô¤n otro descrito en ICAP. SerûôÙa un patrûô°n granular con metafases positivas? |
|
|
AC- |
How to explain a positive antidsDNA (IFA Crithidia luciliae 1:320) with a HEp-2 IFA nuclear dense fine speckled pattern (AC-2)? The HEp-2 pattern was confirmed in two different manufactures, 2 different experienced analists and diluted much more than 1:640. |
|
|
AC- |
I would appreciatte if you could share your opinion about the quasi homogeneous HEp-2 IFA pattern (not yet on the ICAP algorithm) and coment on its IFA morphology. |
|
|
AC- |
Irregular cytoplasmatic staining
Hi, my name is Ana Portu, I am a biochemist and PhD in Immunology (UBA-Argentina). I worked at Hospital Aleman in Buenos Aires until September 2019 and now I continue working in autoimmunity in a smaller city of the same country. My question is about a cytoplasmatic pattern in a serum sample of a 62 year old patient with gottron papules and extreme tiredness. Jo-1 antibody is negative (LIA-Orgentec) and I tried in two different brands of Hep-2 substrates. I would like to send you the pictures that I took from the different wells, in which I observe cytoplasmatix staining similar to AC-19, but not in every cell. I have discussed them with two specialist in my former laboratory and we decided it would be best to ask for your opinion. Thank you.
Dra Ana Ines Portu
BioquûôÙmica - Doctora Area InmunologûôÙa
Argentina |
|
|
AC- |
How would we report mitotic patterns (for example intercellular bridge) if dilution titer is less than 1:320 and higher than 1:100 or week positive (1:100)? Should we report it or not? |
|
|
AC- |
Se puede obtener un resultado de ANA negativo (nûô¤cleo-citoplasma-mitûô°tico) con antûôÙgenos SSA-/Ro, Sm o Jo-1 positivo?? o mûôÀs de alguno de estos antigenos positivos? |
|
|
AC- |
Se puede obtener un patrûô°n AC-2 con algûô¤n antûôÙgeno de perfil ENA positivo?? |
|
|
AC-4 |
<b>Anti-Ro52 antibodies with an AC pattern?</b> Do anti-Ro52 antibodies show any staining pattern matching with known ICAP AC designation? I have a patient with exclusive anti-Ro52 +++ (strong) in immunoblot and I do not know which AC pattern it should correspond to. AC-4? AC-XX? |
<p><p>Anti-Ro52
antibodies (also known as anti-TRIM21) characteristically do not produce a
distinctive staining pattern on commercially prepared HEp-2 cells using the indirect
immunofluorescence assay (HEp-2 IFA). They also do not show reactivity in double
immunodiffusion or classical radioimmunoprecipitation assays. One explanation put
forth is that these autoantibodies recognize predominantly denatured epitopes
in the middle leucine zipper domain, which are poorly available in these
assays. Consistent with this hypothesis
is that anti-Ro52 are readily detected in immunoblot, ELISA and chemiluminescent
immunoassay (CLIA) and bead-based immunoassays. However, it has also been
reported that antibodies to "native" Ro52 were detected in ~50% of anti-Ro52
positive sera using an N-terminal Ring finger domain in an <i>in vitro</i>
translation and immunoprecipitation assay (1). Whether the native
epitope is blocked for antibody access in other immunoassays is unclear. </p>
<p> </p>
<p>If
your anti-Ro52 patient sample presents any reactivity in HEp-2 IFA, it probably
contains additional autoantibodies against antigens other than anti-Ro52. In
other words, samples with exclusive anti-Ro52 reactivity tend to be negative in
HEp-2 IFA. </p>
<p> </p>
<p>1. Buyon
JP, Slade SG, Reveille JD, Hamel JC, Chan EKL. Autoantibody responses to the
"native" 52-kDa SS-A/Ro protein in neonatal lupus syndromes, systemic
lupus erythematosus, and Sjogren's syndrome. <i>J Immunol</i>. 1994 Apr 1;<b>152</b>:3675-84.</p>
</p> |
|
AC- |
Can I have anti-histone antibody with negative pattern in Hep-2 cells with positive mitosis?
Mitosis similar to those observed in the centromere pattern. |
|
|
AC-9 |
<div><b>Discrepancy in HEp-2 IFA and western blot data</b>. How do you explain the detection of antibodies by western blot (WB) that are not related to the pattern observed in HEp-2 cells by indirect immunofluorescence (IFA)? </div> |
<p>This is not an uncommon phenomenon and there are several possible explanations for this apparent discrepancy. <br><br>It is recognized that each immunoassay platform (IFA, WB, ELISA, immunoprecipitation (IP), etc.) is dependent upon a given set of epitopes of relevant autoantigens (1). Broadly, autoantibodies recognize linear and/or discontinuous (native or conformational) epitopes. In the context of discontinuous epitopes, it is important to appreciate that many target autoantigens are part of macromolecular complexes where unique epitopes might be represented as quaternary structures. Immunoassays where the epitope structures are best preserved include IP of cell lysates and HEp-2 IFA. However, there is an important caveat for HEp-2 IFA because the cells have been fixed in methanol and/or acetone (or other undisclosed ûÂã˜ùtrade secretûÂã˜ã fixatives) that likely alter some epitopes as well as well as exposing others. As to the question of native epitope preservation, WB presents the largest challenge because the protocols of boiling proteins under deliberate denaturing conditions most likely alters epitopes significantly. It is true that some may renature/refold after electro-transfer of proteins to nitrocellulose membrane, but many most likely do not. When ûÂã˜éantibodies by blotûÂã˜ô are ûÂã˜énot related to the pattern observed in HEp-2 cells by IFA,ûÂã˜ô one explanation is that antibodies to epitopes recognized in IFA are not identical to or represent only a proportion of those (or even different ones) recognized in a WB. One example for this is anti-fibrillarin; IFA typically shows an AC-9 pattern and yet negative in immunoblot because a high percentage of anti-fibrillarin antibodies do not recognize denatured fibrillarin in immunoblot.<br><br>It is common that a given serum sample (especially in SLE) has more than one autoantibody specificity. Hence, another explanation is that when two (or more) completely different antibody specificities co-exist in the same sera, confounding results can be observed, especially on the HEp-2 IFA. In that case, the HEp-2 IFA pattern may reflect the combination of IFA reactivity of all present autoantibodies and the resultant pattern may be different from the one expected if there were only one autoantibody specificity in the serum.<br><br>1. Mahler M, Bluthner M, Pollard KM. Advances in B-cell epitope analysis of autoantigens in connective tissue diseases. Clin Immunol. 2003 May;107:65-79.<br><br><br></p> |
|
AC- |
If the autoantibodies identified by western blot or elisa are not related to the pattern observed by immunofluorescence should we give this information to the prescribing Doctor?
or if the pattern is very suggestive of a certain autoantibody but we cannot identify it, we should say that it is negative for this autoantibody?
for example: nucleolar pattern suggestive of fibrillarin but not identified by WB.
another exemple Centromere pattern without identification by elisa and WB.
How to give these results?
|
|
|
AC- |
How to give mixed pattern results?
Is a nuclear fine speckled patern with positive mitosis considered a mixed pattern?
|
|
|
AC- |
In some times ANA Negative samples may become positive or visible. How to clarify this issue? |
|
|
AC- |
My name is Rita Monteiro, I am Clinical Patologist responsible for autoimunity in AveiroûôÇs Hospital (Portugal), and I have some patients with ac 23pattern who do not have hepatitis c or exposure to any kind of medication. Do you know other cases of this ac 23 pattern not associated with hepatitis C therapeutic or other types of the therapeutic? Will we be facing a new entity associated with other autoimmune diseases? |
|
|
AC- |
I would like to ask you if you could supply our lab with positive samples for ASMA and AC-1 pattern. |
|
|
AC- |
I would like to know if there is any report on the results of the 5th ICAP workshop, September 2019.
Another question, has some consensus been reached about compound patterns and mixed patterns?.
Thanks a lot,
Juana Jimûôˋnez |
|
|
AC- |
Hello
I am a Biologist, MSc and I would like to ask you if there are any opportunities for training on ANA patterns in certain qualified labs. I have been working in the field the last four years and my aim is to expand my knowledge and experience especially in fluorescence microscopy and ANA patterns to the level of experties
Kind regards
Christina Petropoulou |
|
|
AC- |
I am interested in knowing Ifigenia TeherûôÀn is a y su Mary of agreements in te fifth ICAP workshop of 2020
Thanks a lot, Lola Serrano |
|
|
General |
<p>
<b>What is the magnification needed for assigning HEp-2 IFA patterns?</b><br>Question: Has ICAP made any clear statement about the magnification at which HEp-2 IFA staining patterns in should be evaluated before assigning a pattern?
<br></p> |
<p>Answer: In the literature, there is general acceptance that accurate assessment of IFA patterns on HEp-2 cells requires a minimum total magnification of 400x (40x objective and 10x ocular) when analyzing the slides directly through the microscope. However, a similar statement has not been made by the ICAP Executive Committee. <br><br>Many semi-automated IFA readers use 200x magnification, which is sufficient to allow interpretation of many AC patterns. However, digital images taken on semi-automated instruments (or from traditional microscopes) are different from viewing live images through microscope eyepieces. For images submitted to ICAP, it is recommended that the minimum magnification should be 400x. <br><br>To fully appreciate all the 5 features of AC-29 (topo I-like) and the nuclear tiny speckles of AC-4a, 400x magnification is recommended. A 400x magnification is also needed most of the times to differentiate the nucleolar patterns (AC-8,9,10) and the nuclear envelope patterns (AC-11,12).<br><br><br><br></p> |
|
AC-4 |
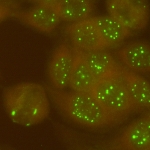
<p><b>Tips to identify AC-31 pattern</b><br>Question: Any good tip to observe AC-31 pattern?<br></p> |
<p>Answer: To appreciate the characteristic myriad tiny dots of the AC-31 nuclear speckled pattern, one should carefully adjust the fine adjustment knob to notice the tiny dots that may be present at slightly different focal planes. The characteristics of AC-31 may not be evident at the screening 1/80 dilution and become clearer as the sample is further diluted. In general, the 400x magnification is appropriate for the identification of the AC-31 pattern characterized by innumerable tiny pinprick-like dots slightly variable in size. In addition, we noticed that AC-31 is more evident with certain HEp-2 slide brands (e.g. Bion-MBL, Aesku, Medipan, BIO-RAD, and Inova) than with others, and this may depend on distinct details of the cell culture and fixation methods applied by different manufacturers. Therefore, one needs to identify how the AC-31 pattern shows up in the particular HEp-2 slide brand in use in the laboratory. The availability of the IUIS/ASC reference serum IS2105 will also help laboratories to identify this AC-31 pattern efficiently. In summary, the best tip for identifying AC4a is to have enough time to devote to reading using a good microscope and not just relying on an automatic reading system.<br><br>References<br><br>Rober N, Dellavance A, Ingenito F, Reimer ML, Carballo OG, Conrad K, Chan EKL, Andrade LEC (2021) Strong association of the myriad discrete speckled nuclear pattern with anti-SS-A/Ro60 antibodies: consensus experience of four international expert centers. Front Immunol 12:730102. DOI: 10.3389/fimmu.2021.730102<br><br>Dellavance A, Alvarenga RR, Rodrigues SH, Barbosa SH, Camilo AC, Shiguedomi HS, Rodrigues SS, Silva CG, Andrade LE (2013) Autoantibodies to 60kDa SS-A/Ro yield a specific nuclear myriad discrete fine speckled immunofluorescence pattern. J Immunol Methods 390:35-40. DOI: 10.1016/j.jim.2013.01.006<br><br></p> |
|
AC- |
Good morning, we encountered a case with suspected ( rods and rings pattern AC 23) see attached file. Please confirm if we are correct, as we didnûÂã˜ãÂt see such pattern before.
Thanks in advance |
|
|
AC- |
Hello
Can you please help me identify the immunofluorescence pattern in Hep-2 cells from the attached image?
How to classify in ICAP nomenclature?
I think it`s a granular cytoplasmic pattern, probably AMA but the anti-M2 and anti-M2-3E test is negative.
Thank you so much,
Arminda GonûôÏalves |
|
|
AC- |
Hello again!
How do you explain the difference in patterns with just a difference title?
In the 1/160 diltution I have a Midbody and "Rods and Rings" patterns and in the 1/320 dilution I see nucleoli.
Should I consider nucleoli positive at the 1/320 dilution (the images are identified with the dilution).
Best regards,
Arminda GonûôÏalves |
|
|
General |
<b>Mitotic patterns are reported as ANA-positive or -negative?</b><br>Question: Should I report positive mitotic patterns as ANA-positive or ANA-negative?<br> |
<p>The short answer to your question is that when mitotic patterns (AC-24 to AC-28) are detected, they should be reported as ûÂã˜éANA positiveûÂã˜ô (see reference below). <br><br>The long answer involves some considerations. We know that there is quite a difference in how mitotic (or even cytoplasmic) patterns are reported depending on the region of the world. Some countries report positive mitotic patterns as ANA+ and others as ANA-. Even within a country, some laboratories may report positive mitotic patterns as ANA+ and others as ANA-. It is important to harmonize your reported test results with the local ûÂã˜ùcultureûÂã˜ã and practices where you reside. Nevertheless, we recommend following the ICAP suggestions at <a target="_blank" rel="nofollow" href="http://www.anapatterns.org">www.anapatterns.org</a>. <br><br>The most important part is to ensure that your ûÂã˜écustomersûÂã˜ô understand your results. ICAP recommends that you avoid using terms like ûÂã˜éANA positiveûÂã˜ô or ûÂã˜éANA negative.ûÂã˜ô In fact, the term ANA is outdated, and we prefer to refer to the actual assay, which is an indirect immunofluorescence assay using HEp-2 slides or HEp-2 IFA, as a transition to a new description for this test: Anti-Cell Antibodies (see reference below).<br> <br>We have been trying to disseminate the concept that there is more in the HEp-2 IFA test than just "positive" or "negative." We know that clinicians (and laboratories) are familiar with this dichotomous concept, but we also learned that clinicians learn fast how to use HEp-2 IFA patterns for better clinical decisions. <br><br>Reference<br>von Mûô¥hlen et al. (2021) How to report the Antinuclear Antibodies (Anti-Cell Antibodies) test on HEp-2 cells: guidelines from the ICAP initiative. Immunol. Res., in press.<br><br><br></p> |
|
AC- |
Si un paciente tiene un resultado:
ANA NEGATIVO
ENA POSITIVO
SCL 70 , JO, SSB, SM, RNP, SSA Y ANTI-DNA NEGATIVO.
A QUE SE DEBE ESTO? |
|
|
AC- |
Female, 69Y.
Newly diagnose small cell lung carcinoma.
On aspirin. Treating with meropenem and vancomycin
ANCA, MPO, PR3 Negative.
Bioplex ANA (dsDNA, Chrom, Ribo P, SSA, SSB, Cent B, Sm, RNP, Jo1, SCL70) all negative.
On Biorad Kallestad HEp-2 slides, we observed positive chromatin bar (>640), dots with variable size (or Coarse Speckled?) (>640), nucleolar (>640), some of the mitotic cells (~20%) got centrioles (>640)
May we know how to interpret and report the ANA slides results? |
|
|
AC- |
Dear ICAP team. I hope you are well. Thank you for the wonderful and insightful work you do. I am wondering on the clinical relevance of a positive ANA test, without ENA antibodies? For example, if the ANA is of a pattern not typically seen in healthy individuals e.g. homogenous, fine speckled, nucleolar and the patient is symptomatic but without ENA- can diagnosis of autoimmune SSE, SjS, DM etc still be possible?
Thank you. Niamh. |
|
|
AC- |
Good morning,
how should I consider a sample which does not show any clear positivity AC11 or AC12 but a strong positivity for gp210 in Immunoblotting? We have performed Immunoblotting for gp210 since the automated microscope has considered the sample positive for this kind of pattern which is not so evident for us on Hep-2 IFI, nor on the rat liver. It seems an AC4 1:80, not very defined. Should we report this positivity for the patient or we should ignore it since it is not confirmed by the IFI?
Thanks a lot for your help.
Dr Laura Cuomo
email: laura.cuomo@aslroma1.it |
|
|
AC- |
In the images of AC-18 section on the website (https://anapatterns.org/view_pattern.php?pattern=18), there are some AC-18 images with cytoplasmic dense fine speckled background.
For example, in the 1st image uploaded, would you recommend reporting AC-18 alone or AC-18 + AC-19 in the cytoplasmic domain?
It seems reasonable clinicians may need to do secondary antibody test to survey if the patient has relevant tRNA synthetases antibodies or ribosomal-P if AC18+AC19 reported but not if AC-18 alone reported. Your suggestions will be of great help to us. Thank you very much!
We also have some clinical images (uploaded images 2 and 3). How do you suggest reporting these images?
|
|
|
AC-5 |
<b>IFA pattern changed from coarse granular to homogeneous </b><div>Question: The HEp-2 IFA pattern of a patient has changed from coarse granular to homogenous after 6 months. Is it possible?<b></b></div> |
<p>With all things being equal, same slide manufacturer with same slide lots, same conjugate, and same serum dilution to ensure there are no technical issues, HEp-2 IFA patterns can change over time. This may include a change from no detectable pattern (AC-0) to any AC pattern and vice-versa. Many factors such as disease progression or overlap syndrome, new interventions (drugs, biologicals), new exposures (infectious disease, cancer, etc.) can also affect such changes. It is important to know if the end-point titer also changed (increased or decreased by at least 2 dilutions).<br>What is the immunological basis for changes in HEp-2 IFA status along the course of SLE? Autoantibody levels do fluctuate along the disease course. Some of them (i.e., native DNA and nucleosome, for example) may fluctuate in relation to disease activity, while others (i.e., anti-Ro60 and anti-Sm) appear to fluctuate independently of disease activity.<br>Can HEp-2 IFA temporal changes be related to disease activity? Most people would say ûÂã˜énoûÂã˜ô, but the answer is not so simple. A recent study from the Andrade lab evaluated 269 SLE patients regarding their HEp-2 IFA titer and pattern in a transverse (active x intermediary x inactive disease activity) and prospective (change in disease activity status in the same patient along 1-year follow-up) (1). The report showed that patterns and titer change can change and there was some association with disease activity status. High titer and the AC-1 pattern were associated with active disease, whereas low titer and the AC-4 pattern were associated with disease remission. Interestingly, the diagnostic performance (ROC curve AUC) of HEp-2 titer for the definition of disease activity was in the range of traditional disease activity biomarkers (anti-dsDNA, anti-nucleosome) and much greater than C3 and C4. However, the HEp-2 IFA is not recommended as a test for monitoring SLE disease activity. Similar conclusions may apply to other ANA-related rheumatic diseases. <br>Thus, coming back to the index case, the change from AC-5 to AC-1 may indicate the appearance of anti-nucleosome and/or anti-dsDNA antibodies. It is recommended to be aware of these autoantibodies and possible disease flare.<br>1. Prado MS, Dellavance A, Rodrigues SH, Marvulle V, Andrade LEC (2020) Changes in the result of antinuclear antibody immunofluorescence assay on HEp-2 cells reflect disease activity status in systemic lupus erythematosus. Clin Chem Lab Med 58:1271-1281. DOI: 10.1515/cclm-2019-0638<br><br><br><br></p> |
|
AC-1 |
<b>Low titer anti-dsDNA serum negative by HEp-2 IFA?</b><br>Question: Can I have a negative HEp-2 IFA result in a sample with positive Crithidia assay at 1/20? The negative HEp-2 IFA was confirmed with slides from different commercial brands.<br> |
<p>Answer: In most cases, a sample with anti-dsDNA antibodies is associated with a homogeneous nuclear pattern (AC-1). In rare occasions, no nuclear staining is observed and that happens because the DNA epitopes recognized by the antibodies in that sample are present in the highly compacted Crithidia luciliae kinetoplast DNA, but not in commercially-prepared HEp-2 cells that are commonly used. In those cases, it may be helpful to do the HEp-2 IFA test with another HEp-2 kit, which may or may not be positive. In your case, it is clear that you have confirmed the negative result in different commercial kits. In some cases, the anti-dsDNA antibodies target DNA epitopes that are hidden by interaction with histones and other proteins (e.g., high mobility group proteins) in the nucleus. In such cases, extraction of histones and other nuclear proteins with 0.1N HCl prior to the IF reaction may allow the anti-dsDNA antibodies to produce the expected AC-1 pattern. Finally, it must be certified that the immunofluorescence reaction that you observed in the Crithidia assay corresponds to the kinetoplast and not to the basal body. <br></p> |
|
AC- |
<b>Reporting AC-18 - does it change with the 2021 classification chart revision?</b><br>Question: I have one question for the new classification tree. As AC-18 was removed from the category of cytoplasmic speckled and assigned still at the expert level. If the lab only reports competent-level patterns, how should AC-18 be reported? Should they just report the first branch of the classification tree as "cytoplasmic"?<br> |
<p>Answer: The competent-level designation is ideally aimed at laboratories starting to train on reading HEp-2 IFA patterns and they can focus on covering all the competent-level patterns first. In other words, the competent-level covers all patterns considered essential to be reported by a laboratory testing for HEp-2 IFA. However, ICAP is not implying that labs should stop there with a ûÂã˜édonûÂã˜ãÂt cross this lineûÂã˜ô thinking.<br><br>Thus, if a lab can recognize AC-18 (cytoplasmic discrete dots), they can just report it as AC-18. How should we consider a lab being competent with AC-18? It would be ideal that they establish an internal standard reference for AC-18 (based on external reference material as provided by the IUIS autoantibody standardization committee <a target="_blank" rel="nofollow" href="https://asc.dental.ufl.edu/reference-sera/">https://asc.dental.ufl.edu/reference-sera/</a>) and check their HEp-2 substrate whenever they have new batches. This ensures that they should be able to recognize AC-18.<br><br>If a lab does not recognize AC-18 by the above policy/reference, they can report just as cytoplasmic.<br><br></p> |
|
AC-4 |
<b>True IFA staining masked at low dilution? </b><div>Question: In the IFA testing of a 9-year-old female lupus patient, initial dilution at 1/40 produced a bright fuzzy cytoplasmic staining with no well-defined pattern. Surprisingly nuclear fine speckled AC-4 was observed at 1/160. Is it common that the cytoplasmic staining completely masked the nuclear staining at low dilution?</div> |
<p>Answer: This is a phenomenon that not many people are aware of, but it may occur in some practice. Some samples at low dilution yield an apparently negative HEp-2 IFA result and as we dilute the sample there is a progressive appearance of a nice and defined reactivity. This does not mean we should titer every sample with a negative result at 1/80, but it may be worthwhile to give it a try for those that produce a bright fuzzy staining (no defined pattern) at 1/80. Failure to be aware of this potential problem may account for false-negative results in some cases.<br></p> |
|
General |
<p>
<b>Differences between multiple, mixed, and composite HEp-2 IFA patterns?</b><br>Question: Can you provide more information on how ICAP defines the differences between multiple patterns, mixed patterns, and composite patterns in HEp-2 IFA?
<br></p> |
<p>Answer: We refer to simple patterns when we observe single and isolated clear-cut HEp-2 IFA patterns, e.g. AC-23 or AC-3. The terms multiple, mixed, and composite IFA patterns refer to close but distinct concepts that go beyond the simple patterns. <br>1. The term "multiple patterns" applies to situations where two or more individual and clearly discernable patterns, e.g. AC-1 + AC-23 or AC-4 + AC-22, are observed in an individual serum sample (i.e., each of the patterns is clearly identified). <br>2. The term "mixed patterns" applies to observations where a serum sample produces more than one pattern in the same cell compartment and it is not possible to clearly identify each of the components. As an example, AC-4 + AC-5 can commonly be seen together but we are unable to distinguish each of the components (AC-4 and AC-5); in those cases, the HEp-2 IFA staining pattern is regarded as a mixed nuclear-speckled pattern. <br>3. Finally, the term "composite patterns" is applied to cases in which a single antibody causes staining of two or more cell compartments and the composite image is so characteristic that it always evokes the presence of that autoantibody. For example, the AC-26 pattern is an interphase nuclear staining pattern accompanied by mitotic spindle fiber staining and is typically associated with anti-NuMA antibodies. Similarly, the AC-14 pattern, typically associated with anti-CENP-F antibodies, is characterized by nuclear fine speckled staining with variable intensity in interphase cells, a delicate centromere staining only in mitotic cells, staining of the inter-cellular bridge, and nuclear envelope staining exclusively in prophase cells.<br><br></p> |
|
AC- |
Sharing with you one pattern i just saw from my last reading. |
|
|
AC- |
is it possible fana positive and immunoblotting negative?i have pation with 1:1000 coarse speckel in cytoplasm and weak fine granular in nucleoplasm but ana profile (immunoblot is negative ) is it possible? |
|
|
AC- |
i cant detection this pattern , can help me ? |
|
|
AC- |
Anti PCNA antibodies captured in western blot but IIFT screen negative. Can u explain. |
|
|
AC- |
A serum sample is showing Speckeld pattern in IIFT ANA but western blot negative. Kindly explain |
|
|
AC- |
can you help us identify this pattern? |
|
|
AC- |
can you help me to identify this pattern? |
|
|
AC- |
can you help me identify this pattern? i submitted 3 images. the manufacturer is euroimmun. the images were taken from hep 2 rat. we used 1:40 dilution. |
|
|
AC- |
I would like to submit to your attention a pattern that I have never seen,
the patient declares that his clinical diagnosis has been cutaneous LES and that he has just cutaneous symptoms that can be controlled with cortisone. We thought that it could be ascribed to antibodies anti-HMGCR which is linked to necrotising myositis, but the liver does not show the typical pattern, CK of the patient on the other hand is normal, not elevated.
Do you have some experience for this pattern? Or any suggestion to elucidate its origin? Thanks for your attention and your help. I enclosed three images of the pattern on Hep-2 and rat liver.
Waiting for your support,
best regards
Laura Cuomo (M.D. San Filippo Neri Hospital, Rome) |
|
|
AC- |
Dear all,
how should you classify this pattern on HEp-2 (2 different patients) ? I can send you some other images on rat tissue slides, the pattern is like anti-ribosome or SRP antibodies, so discrepancy with the HEp-2 cytoplasm which is reticulated. Could it be a peculiar anti-reticulum antibody ?
Thanks for your HElp,
kind regards
JL Charuel |
|
|
AC- |
Hello.
I have found this interesting pattern in several of our patients, but we cannot determine the specific antigen. It looks like it could be antibodies against a cytoskeleton element, but HEp-2 cells appear to be negative for the cytoplasm. I include three images (HEp-2, rat liver and rat stomach from Euroimmun) from the same patient. I would really appreciate if you could shed some light to this finding.
Thank you. |
|
|
AC- |
Hello.
I have found this interesting pattern in several of our patients, but we cannot determine the specific antigen. It looks like it could be antibodies against a cytoskeleton element, but HEp-2 cells appear to be negative for the cytoplasm. I include three images (HEp-2, rat liver and rat stomach from Euroimmun) from the same patient. The IFA pattern does not change with serial dilutions. I would really appreciate if you could shed some light to this finding.
Thank you. |
|
|
AC- |
Hello.
I have found this interesting pattern in several of our patients, but we cannot determine the specific antigen. It looks like it could be antibodies against a cytoskeleton element, but HEp-2 cells appear to be negative for the cytoplasm. I include three images (HEp-2, rat liver and rat stomach from Euroimmun) from the same patient. The IFA pattern does not change with serial dilutions. I would really appreciate if you could shed some light to this finding.
Thank you. |
|
|
AC- |
Hello.
I have found this interesting pattern in several of our patients, but we cannot determine the specific antigen. It looks like it could be antibodies against a cytoskeleton element, but HEp-2 cells appear to be negative for the cytoplasm. I include three images (HEp-2, rat liver and rat stomach from Euroimmun) from the same patient. The IFA pattern does not change with serial dilutions. I would really appreciate if you could shed some light to this finding.
Thank you. |
|
|
AC- |
Hello.
I have found an interesting IFA pattern in some of the patients of my centre. It seems like autoantibodies are directed against the cytoskeleton, but interestingly, HEp-2 are cytoplasm negative. I include three images (HEp-2, rat liver and rat stomach form EUROIMMUN) from one of the patients. The IFA pattern does not change on serial dilution. I would really appreciate if you could shed some light on this finding.
Thank you. |
|
|
AC- |
Hello.
I have found an interesting IFA pattern in some of the patients of my centre. It seems like autoantibodies are directed against the cytoskeleton, but interestingly, HEp-2 are cytoplasm negative. I include three images (HEp-2, rat liver and rat stomach form EUROIMMUN) from one of the patients. The IFA pattern does not change on serial dilution. I would really appreciate if you could shed some light on this finding.
Thank you.
|
|
|
AC- |
Hello.
I have found an interesting IFA pattern in some of the patients of my centre. It seems like autoantibodies are directed against the cytoskeleton, but interestingly, HEp-2 are cytoplasm negative. I include three images (HEp-2, rat liver and rat stomach form EUROIMMUN) from one of the patients. The IFA pattern does not change on serial dilution. I would really appreciate if you could shed some light on this finding.
Thank you.
|
|
|
AC- |
Hello.
I have found an interesting IFA pattern in some of the patients of my centre. It seems like autoantibodies are directed against the cytoskeleton, but interestingly, HEp-2 are cytoplasm negative. I include three images (HEp-2, rat liver and rat stomach form EUROIMMUN) from one of the patients. The IFA pattern does not change on serial dilution. I would really appreciate if you could shed some light on this finding.
Thank you.
|
|
|
AC- |
Hello.
I have found an interesting IFA pattern in some of the patients of my centre. It seems like autoantibodies are directed against the cytoskeleton, but interestingly, HEp-2 are cytoplasm negative. I include three images (HEp-2, rat liver and rat stomach form EUROIMMUN) from one of the patients. The serum dilution is 1:160 and the IFA pattern does not change on serial dilution.
I would really appreciate if you could shed some light on this finding.
Thank you.
|
|
|
AC- |
I am an editor of a textbook for Japanese students who are aiming to laboratory technologists. When I revise the ANA section, can I get permission to use some of the pictures downloaded from ICAP website? Or, do you think it is too early to explain ANA IIF patterns following the ICAP classification, which has not been the universal standard, in a textbook for undergraduate students? |
|
|
AC- |
I wonder if there are possible to buy a "book" with these patterns (pictures and descriptions). It`s practical to have a "book" nearby the microscope to look up on patterns when you are unsure about something.
|
|
|
AC- |
Estoy muy preocupada con los reportes que se vienen realizando no solo en mi pais sino tambiûôˋn en otros, en cuanto a las diluciones, ya que solo estûôÀn haciendo la 1/80 y no hacen mas diluciones, estûôÀn reportando las aproximaciones que dan dan los equipos, ejemplo si el equipo dice un aproximado de 1/320, sin realizarlas las dan como resultado y las reportan al medico , me preocupa mucho, desearûôÙa su opiniûô°n |
|
|
AC- |
Hello, I work in a laboratory and want to do the training, allthough its a very good training for my collegues. I know, that some translations are in prozess. I am a german, so its more easier to do the training in german. Can you tell me, when a gernan translation will come.
Thanks a lot!
The homepage is great!! |
|
|
AC- |
I am an editor of a textbook for Japanese students who are aiming to laboratory technologists. When I revise the ANA section, can I get permission to use some of the pictures downloaded from ICAP website? Or, do you think it is too early to explain ANA IIF patterns following the ICAP classification, which has not been the universal standard, in a textbook for undergraduate students? |
|
|
AC- |
Is it possible to access the information in the ICAP training programme, once completed and passed the multiple choice exam. There is lots of useful information in there that I would like to re-visit. Thank you, Janine Dixon |
|
|
AC- |
In nucleolar patterns I can rarely (when there are tests) identify the associated autoantibody.
How important is this identification?
|
|
|
AC- |
Can I say that in the AC-5 pattern with negative U1RNP, Sm and RNA Polimerase III autoantibodies, the hnRNP can be positive? |
|
|
AC- |
In daily practice, I often observe granular and fine granular patterns with positive metaphase plaque without identification of any antibody (Immunoblot with nucleosomes, histones, SS-A, Ro-52, SS-B, nRNP/Sm, Sm, Mi-2a, Mi-2b, Ku, CENP A/ B, Sp100, PML, Scl-70, PM-Scl 100/ 75, RP11/ 155, gp210, PCNA and DFS70), even with high titles.
By definition granular patterns AC-4 and AC-5 do not have the chromatin marked.
What ICAP id should I give?
Where to fit this pattern? |
|
|
AC- |
Estimados, querûôÙa consultar por un patrûô°n de fluorescencia que no pudimos clasificar, el mismo se observa como un AC-27 Puente intercelular, pero ademûôÀs se visualizan algunas cûôˋlulas en interfase positivas (con tinciûô°n nuclear y nucleolar), similar a un patrûô°n pleomûô°rfico. Esa figura fue observada hasta una diluciûô°n 1/320 del suero en HEp-2 de BIO-RAD. AgradecerûôÙa alguna referencia y si corresponderûôÙa informarlo como un patrûô°n AC-XX. Paciente femenina de 40 aûôÝos con MiopatûôÙa en estudio. Se Adjuntan imûôÀgenes.
Muchas gracias
|
|
|
AC- |
Hola,Tenemos una muestra de un paciente, que se le realizo dilucion 1:80, 1:160 y 1:1280, el resultado fue confuso ya que observamos todo el fondo fluorescente (que no corresponde a ningun patron citoplasmatico), suponemos que deben ser anticuerpos que se estûôÀn uniendo de manera inespecifica, nos pueden orientar un poco?
Adjuntos imagenes |
|
|
AC- |
Hello, I have a question about a test that we have repeated twice with a different sample from the same patient. When we analyze 1:80 and 1:160 dilutions, we observe a fluorescence in the entire the background. This fluorescence is not a cytoplasmic pattern, we think it may be antibodies that are joining in an unspecific way.
I hope you can help us with this case, she is a 56-year-old female patient, it is the second time that we ask for a new sample, since we have not been able to have a result, I attach the images of the dilutions.
Thank you |
|
|
AC- |
If a sample has a mixed pattern e.g. homogenous and nucleolar at a screening titre of 1/80 but only has nucleolar pattern visible at higher titres( 1/200, 1/400), is there a consensus on how this should be reported? Nucleolar plus the titre(excluding homogenous in final report) homogenous and nucleolar plus the final titre (despite this not being the relevant titre for the homogenous pattern) or both patterns and relevant end point titre for each, reported? |
|
|
AC- |
If a sample has a mixed pattern e.g. homogenous and nucleolar at a screening titre of 1/80 but only has nucleolar pattern visible at higher titres( 1/200, 1/400), is there a consensus on how this should be reported? Nucleolar plus the titre(excluding homogenous in final report) homogenous and nucleolar plus the final titre (despite this not being the relevant titre for the homogenous pattern) or both patterns and relevant end point titre for each, reported? |
|
|
AC- |
If a sample has a mixed pattern e.g. homogenous and nucleolar at a screening titre of 1/80 but only has nucleolar pattern visible at higher titres( 1/200, 1/400), is there a consensus on how this should be reported? Nucleolar plus the titre(excluding homogenous in final report) homogenous and nucleolar plus the final titre (despite this not being the relevant titre for the homogenous pattern) or both patterns and relevant end point titre for each, reported? |
|
|
AC- |
Why does ICAP not adopt the Brazilian Consensus?
In the routine laboratory, mixed, compound or multiple patterns are frequently observed. |
|
|
AC- |
Hello, is it normal to found antiDNA antibodies with high titer in Elisa without finding the homogeneous pattern in HEP-2 IFA??
Would you telling me how to report the result? thank you |
|
|
AC- |
Buenas noches, puede ocurrir el caso de ver fluorescencia muy fuerte en anti dsDNA pero con ANA negativo? |
|
|
AC- |
Buenas noches, puede ocurrir el caso de ver fluorescencia muy fuerte en anti dsDNA pero con ANA negativo? |
|
|
AC- |
Buenas noches, puede ocurrir el caso de ver fluorescencia muy fuerte en anti dsDNA pero con ANA negativo? |
|
|
AC- |
Puede presentarse un tûôÙtulo alto de dsDNA con ANA negativo |
|
|
AC- |
Puede presentarse un tûôÙtulo alto de dsDNA con ANA negativo |
|
|
AC- |
Under what conditions can a very positive dsDNA test with negative ANA occur?. What processing conditions can I carry out to confirm said result? |
|
|
AC- |
What do you do of the classified the U1-70snRNP |
|
|
AC- |
What donûÂã˜ãÂt you of the classified U1-70snRNP |
|
|
AC- |
what is the difference between the scpet AC-19 and the associated antigens U1-70snRNP |
|
|
AC- |
what is the difference between AC- 19 and associated antigen U1-snRNP
|
|
|
AC- |
What is the difference between AC-9 and the associated antigen U1 -snRNP |
|
|
AC- |
What aspect is associated with antigen U1-snRNP |
|
|
AC- |
What is aspect is associated with antigen U1-snRNP |
|
|
AC- |
What is antigen is associated with aspect |
|
|
AC- |
what is antigen between |
|
|
AC- |
what is antigen associes or actine |
|
|
AC- |
How multiple, mixed, and composite HEp-2 IFA patterns should be report? |
|
|
AC- |
Dear Sir/ Mam,
we have observed a pattern twice which has a nuclear smooth envelop like interphase cells (AC 11) but with metaphase plate has stained positive. we have confusion in assigning AC pattern and numbers for such cases.
we are performing ANA on Hep2 substrate manufactured by Inova diagnostics.
we have not observed a pattern change with dilution.
we perform the tests at 1:40 dilution as per the manufactures kit instructions.
we have provided two images of the same case. request your expert guidance in approaching such cases.
Thank you.
Regards. |
|
|
AC- |
Dear Sir/ Mam,
we have observed a pattern twice which has a nuclear smooth envelop like interphase cells (AC 11) but with metaphase plate has stained positive. we have confusion in assigning AC pattern and numbers for such cases.
we are performing ANA on Hep2 substrate manufactured by Inova diagnostics.
we have not observed a pattern change with dilution.
we perform the tests at 1:40 dilution as per the manufactures kit instructions.
we have provided two images of the same case. request your expert guidance in approaching such cases.
Thank you.
Regards. |
|
|
AC- |
Cûô°mo informan los Anti ccp, que en la ifi se ve como una imagen moteada con metafses positivas pero que no es ni un Ac1 no un un AC-2? |
|
|
AC- |
DNA positivo en pacientes chagasicos, con fan negativo? Cûô°mo informarlo? |
|
|
AC- |
Hello. I would like to consult on ANA pattern identification using HEp2 cells and primate liver substrate (EUROIMMUN AG). It seems like speckle patterns and Dense fine speckle patterns are observed in HEp2 cells, but the liver substrate shows no fluorescent on the nucleus. Could you please kindly suggest this? |
|
|
AC- |
How long is it recommended to repeat the ANA HEP-2 test? |
|
|
AC- |
How long is it recommended to repeat the ANA HEP-2 test? |
|
|
AC- |
El Gen UBA1 tiene informaciû°n? |
|
|
AC- |
Dear ICAP-Team,
first, thank you very much for providing this website which i very appreciate.
I am rheumatologist in Berlin, Germany with special interest in laboratory diagnostics.
1)
For each antibody that can induce a characteristic AC pattern, could you please provide the true sensitivity to induce the AC pattern on HEp2 cells (with references, expert opinion if applicable) on your webpage?
Example:
A) Anti-dsDNA antibodies induce a homogeneous nuclear pattern in > 99 %. Consequence: 2-fold elevated anti-dsDNA antibodies in ELISA at AC-0 are very likely a false-positive ELISA result.
B) Anti-PL7 antibodies induce a dense fine speckled or perinuclear cytoplasmic pattern in approx. 40 %.
Consequence: PL7 +++ in myositisblot despite abscense of AC-19 is well compatible with an anti-synthetase syndrome in a patient with rapid progressing pneumonia.
If this information were given, then everyone could quickly recognise for which antibodies IFT on HEp2 cells is a suitable plausibility check.
Or is there something against this that I am not aware of?
2) I could not even clarify in the first report of PL7 in 1984 what the name PL7 is derived from. I only know the word origin for a few autoantibodies (MDA-5, ribP, Sm, dsDNA). Especially for anti-syntethase antibodies, unfortunately, nothing at all can be found. Does anyone from the ICAP group know what the names
Jo1, PL7, Pl12, EJ, OJ, , KS, ZO, Ha, YRS, SC, JS derive from?
Thank you and best regards,
Robert Biesen |
|
|
AC- |
Buongiorno, sono un ragazzo di 19 anni. Mi devo preoccupare quando dice esito dubbio. Cosa vuol dire icap(ac 0) e perchûˋ dice di fare la ricerca per antigeni specifici.
Grazie mille |
|
|
AC- |
Buongiorno, sono un ragazzo di 19 anni. Mi devo preoccupare quando dice esito dubbio. Cosa vuol dire icap(ac 0) e perchûˋ dice di fare la ricerca per antigeni specifici.
Grazie mille |
|
|
AC- |
Buongiorno, sono un ragazzo di 19 anni. Mi devo preoccupare quando dice esito dubbio. Cosa vuol dire icap(ac 0) e perchûˋ dice di fare la ricerca per antigeni specifici.
Grazie mille |
|
|
AC- |
Hi,
This is vamsi krishna from india , i have a quary regarding ANA Pattern, i am using Immuneconcepts hep 2000 cell line.
what can i report cytoplasmic pattern is Positive or Negative,
please let me know it will use for me, i am attaching the images here |
|
|
AC- |
What is the proper format for reporting ANA report ,eg,by IF microscope there is nuclear specked pattern AC-4 .How the report will be |
|
|
AC- |
How to report the suggestive confirmatory tests and follow up tests |
|
|
AC- |
I would like to ask, which pattern would you report for this case.
I attach two photos of HEp-20-10 and one photo of Primate liver cells. Dilution 1:100.
Patient has no earlier clinical history.
Thank you! |
|
|
AC- |
How to become a member of ICAP |
|
|
AC- |
Hello, I am a 25 year old woman and I have been suffering from various symptoms for 2 years; muscular pains in my thighs, tingling in my knees, swelling of the veins in the palms of my hands + pains, small round red spots on my arms, sensation of skin that hurts when it comes into contact with the air and clothing, feeling of burning water when it is cold. These symptoms come and go and then come back. I have positive connectivity ANA = 1:1000 speckled type but negative antigens and a normal inflammatory blood test. A normal electromyogram too.
What do you think???
|
|
|
AC- |
Hello, I am a 25 year old woman and I have been suffering from various symptoms for 2 years; muscular pains in my thighs, tingling in my knees, swelling of the veins in the palms of my hands + pains, small round red spots on my arms, sensation of skin that hurts when it comes into contact with the air and clothing, feeling of burning water when it is cold. These symptoms come and go and then come back. I have positive connectivity ANA = 1:1000 speckled type but negative antigens and a normal inflammatory blood test. A normal electromyogram too.
What do you think???
|
|
|
AC- |
Hello, I am a 25 year old woman and I have been suffering from various symptoms for 2 years; muscular pains in my thighs, tingling in my knees, swelling of the veins in the palms of my hands + pains, small round red spots on my arms, sensation of skin that hurts when it comes into contact with the air and clothing, feeling of burning water when it is cold. These symptoms come and go and then come back. I have positive connectivity ANA = 1:1000 speckled type but negative antigens and a normal inflammatory blood test. A normal electromyogram too.
What do you think???
|
|
|
AC- |
Hello, I am a 25 year old woman and I have been suffering from various symptoms for 2 years; muscular pains in my thighs, tingling in my knees, swelling of the veins in the palms of my hands + pains, small round red spots on my arms, sensation of skin that hurts when it comes into contact with the air and clothing, feeling of burning water when it is cold. These symptoms come and go and then come back. I have positive connectivity ANA = 1:1000 speckled type but negative antigens and a normal inflammatory blood test. A normal electromyogram too.
What do you think???
|
|
|
AC- |
Hello, I am a 25 year old woman and I have been suffering from various symptoms for 2 years; muscular pains in the thighs, tingling in the knees, swelling of the veins in the palms of the hands + pain, small round red spots on the arms, burning sensation in the skin when in contact with the air or clothing, sensation of burning water when it is cold.
I have positive ANA 1:1000 type speckled but antigens all negative. I have a normal inflammatory blood test and a normal electromyogram (EMG).
What do you think? |
|
|
AC- |
<div><b>When anti-SS-A/Ro was lowly positive and changed to negative?</b><br></div>A sample was weakly positive for ANA and anti-SS-A/Ro test last year and now it is negative. Is it possible? Is anti-SS-A/Ro indicative of SjûÑgrenãs syndrome? |
<p>It is not uncommon that ANA (or HEp-2 IFA) positivity can change over time. This may be especially true when the first test showed weak reactivity, as it was in this case. Such fluctuations between positive and negative are common in cases with weak reactivity and can simply be the result of the variability of the IFA technique itself. The serum levels of anti-SS-A/Ro antibodies can also fluctuate over time (1).</p><p><br>It should be noted that anti-SS-A/Ro often includes two distinct autoantibodies that recognize 60kD (Ro60) and 52kD (Ro52) antigens. To ensure reactivity is detected in a sensitive manner, ideally solid phase specific assays for Ro52 and Ro60 should be included, next to HEp-2 IFA to complete the analysis.</p><p><br>The other issue relevant to the result for anti-SS-A/Ro that was positive last year is its clinical significance. Anti-SS-A/Ro antibodies occur in diseases, such as lupus and SjûÑgrenôÇs syndrome. The prevalence of anti-Ro52 autoantibodies is similar to that of anti-Ro60 in every connective tissue disease cohort except for myositis, where anti-Ro52 is common but not anti-Ro60. Occasionally, anti-SS-A/Ro may also occur in people with no apparent disease.<br><br>It is very important to keep in mind that the autoantibodies, by themselves, are not sufficient for the diagnosis of any disease. It is important that the physician match the results of the autoantibody tests with the entire clinical picture of the patient to come to an appropriate diagnosis. <br><br>1.Faria AC, Barcellos KSA, Andrade LEC: Longitudinal oscillation of antibodies to extractable nuclear antigens in systemic lupus erythematosus. J Rheumatol 32: 1267-72, 2005.<br><br></p> |
|
AC- |
<b>How to deal with just a ãnuclear speckledã IFA report?</b><div><b></b>In my practice I have followed patients with ANA findings, with a nuclear speckled pattern (without specifying whether fine/dense/coarse), in patients with very heterogeneous phenotypes, some with a clinical picture that suggests further investigation of systemic autoimmune disease (one patient with proximal muscle weakness and skin thickening) and others who represent only non-specific findings. In such situations, as a precaution, I request more specific autoantibodies. However, this pattern (nuclear speckled pattern) is not described by the "ICAP" and I am in doubt about which antigenic association it represents, even to guide which autoantibody may be present and which ones to look after. How to interpret this pattern? Does the lab describe it when it is not possible to "refine" such a conclusion? Could this be associated with deficiency in the methodology, sample, interpretation?<b><br></b></div> |
<p>The term "nuclear speckled" is an overarching competent- HEp-2 IFA pattern that includes both fine speckled (AC-4) and large/coarse speckled (AC-5). In some cases, it can be difficult to define precisely the speckled pattern a sample produces, being either the fine or large/coarse speckled pattern. Obviously, one may use the ICAP competent level terminology AC-4/5. In such case, one may combine the antibody targets and clinical relevance of the individual patterns, i.e., AC-4 and AC-5. Using the competent level AC-4/5 term may also be appropriate in mixed patterns caused by more than one autoantibody specificity in the sample. <br>Ideally, one should provide the most complete definition of the pattern (expert level), because these provide more specific information on antigenic associations and clinical relevance. For example, as indicated in the "antigen association section" of ICAP website, the nuclear coarse speckled pattern (AC-5) is associated mainly with anti-Sm and anti-U1-RNP antibodies, whereas the nuclear fine speckled pattern (AC-4) has a broader target antigen association. In the ICAP Note #2, AC-4 can be further divided into fine speckled with myriad discrete tiny dots (AC-4a), or simple fine speckled (AC-4b). These are defined patterns and have respective antibody targets, immunological associations, and clinical relevance. The nuclear dense fine speckled pattern (AC-2), on the other hand, should be distinguished from the nuclear speckled patterns AC-4 and AC-5 based on the positive staining of the metaphase plate. With exception of the centromeric pattern (AC-3), the clinical relevance of all patterns is only indicated if the antibody target has been identified. <br><br></p> |
|
AC- |
<p><b>Anti-PCNA positive by blot and yet negative in HEp-2 IFA?<br></b>Can you explain when anti-PCNA antibodies is positive in immunoblot and yet negative in HEp-2 IFA?<b><br></b></p> |
<p>Traditional assays for anti-PCNA are double immunodiffusion and HEp-2 IFA. Positive anti-PCNA antibodies as defined by these assays are probably high titer and are associated with SLE. The ãnewã assays for anti-PCNA using ELISA, Line/Dot blot, CLIA, FEIA, ALBIA, and other solid-phase methods typically detect lower titer (or lower avidity) positives (e.g., higher sensitivity than IFA and immunodiffusion) and this may explain why studies using these methods no longer show a specific association of anti-PCNA with SLE (Vermeersch et al, 2009). More studies are needed on this topic. <br><br>A second consideration with anti-PCNA antibodies is that their reactivity has been reported to be highly dependent on the oxidation status of PCNA in the HEp-2 substrate (Tsai et al, 1992). The initial fascinating observation was that if the HEp-2 slide is taken out from the nitrogen-sealed packet at room temperature for 15-30 minutes before starting the first incubation of the diluted serum in the typical IFA protocol, the anti-PCNA staining was negative or substantially reduced while other ANA were not apparently affected. This loss of reactivity to PCNA was apparently due to air oxidation. The report showed that the free thiol group(s) on PCNA is important for anti-PCNA reactivity of samples from SLE patients. Thus, back to the question, the ãnegative (result) in HEp-2 IFAã would have to be considered more carefully by processing the slide immediately after opening the sealed packet, by using at least one additional HEp-2 slide brand, and by confirming the expected HEp-2 IFA AC-13 pattern with an available reference anti-PCNA serum. <br><br>Please note that there have not been any known recent reports that reproduced the data on the oxidation status-dependency of anti-PCNA staining as reported by Tsai et al. ~30 years ago. This is important because HEp-2 substrate processing, stabilization and fixation may have changed since then. In summary, anti-PCNA reactivity in a solid phase assay accompanied by the typical AC-13 pattern may be more specific for SLE compared to a positive reaction in solid phase assays alone.<br><br>References<br>Vermeersch P, De Beeck KO, Lauwerys BR, Van den Bergh K, Develter M, Marien G, Houssiau FA, Bossuyt X (2009) Antinuclear antibodies directed against proliferating cell nuclear antigen are not specifically associated with systemic lupus erythematosus. Ann Rheum Dis 68:1791-1793. DOI: 10.1136/ard.2008.104190<br><br>Tsai WM, Roos G, Hugli TE, Tan EM (1992) Influence of free thiol group(s) on autoantibody-defined epitope of proliferating cell nuclear antigen. J Immunol 149:2227-2233.<br><br>Mahler M, Miyachi K, Peebles C, Fritzler MJ. The clinical significance of autoantibodies to the proliferating cell nuclear antigen (PCNA). Autoimmun Rev. 2012 Aug;11(10):771-5.<br><br>Mahler M, Silverman ED, Fritzler MJ. Novel diagnostic and clinical aspects of anti-PCNA antibodies detected by novel detection methods. Lupus. 2010 Nov;19(13):1527-33.<br><br></p> |
|
AC- |
Bonjour, une femme de 25ans prûˋsente des symptûÇmes divers depuis 2 ans ; douleurs musculaires aux cuisses, fourmillements genoux, enflure des veines de la paume des mains + douleurs, petite taches rondes rouges aux bras, sensation de brû£lure a la peau au contact de lãair ou des vûˆtements, sensation dãeau brû£lante alors quãelle est froide.
Les ANA sont positifs 1:1000 type mouchetûˋ mais les antigû´nes tous nûˋgatifs. Elle a un bilan sanguin inflammatoire normal et un ûˋlectromyogramme (EMG) normal.
Pas dãantûˋcûˋdents cliniques
Quãen pensez vous ? |
|
|
AC- |
<p><b>How best to recognize the metaphase plate?</b><br>Question: As a new person learning HEp-2 IFA, is there any good tip to identify whether the metaphase plate is positive or negative?<br></p> |
<p>Recognizing mitotic cells and the metaphase plate is an important step in learning to read and interpret HEp-2 IFA. The metaphase plate is like a special place in a cell where all the chromosomes line up perfectly along the middle, making sure everything is ready for the cell to divide, a phenomenon that occurs during the metaphase stage of the cell cycle. Therefore, the metaphase plate primarily contains the autoantigens that belong to chromosomes. The first step is to identify the cells in mitosis. If you use a conjugate that contains DAPI or Hoechst for DNA counterstain, you should be able to recognize metaphase cells using the appropriate filter, as shown in Figure 1.</p><img src="http://www.anapatterns.org/img/faq/fig1.jpg"><br><br><p>Alternatively, you can train yourself in the recognition of cells in metaphase using well-characterized serum samples. For example, select a sample with anti-double-stranded DNA antibodies that produce a clear-cut homogeneous nuclear pattern (AC-1). You will see that the majority of cells will exhibit homogeneous staining within the nucleus during the interphase. Cells in metaphase, however, are less common and you might see only one in every 40X view. These cells look different because they have a specific intense staining of the metaphase plate in absence of staining of the rest of the cell's components. This staining phenomenon of the homogeneous pattern arises due to the integral presence of DNA within the chromosomes. In contrast, a sample with anti-U1RNP antibodies should yield the coarse speckled nuclear pattern (AC-5) in the interphase cells, whereas the metaphase cells present a dark transversal band (not stained) at the cellãs "equator". This is the negative metaphase plate (not stained), because U1RNP is not a chromosomal component. Figure 2 clearly illustrates positive and negative metaphase plates.</p><img src="http://www.anapatterns.org/img/faq/fig2.jpg"><br> |
|
AC- |
El patrû°n homogûˋneo o difuso a que se asocia? |
|
|
AC- |
Our Lab is having a difficult time distinguishing between patterns that are AC-2 DFS and patterns that are mixed homogenous and speckled. We had been told by the manufacturers that DFS has rough looking resting cells and striated mitotics. Homogenous and Speckled mixed patterns should have a fluorescent haloing around the mitotics. Unfortunately, our patients have very ambiguous patterns and exist on a sliding scale of both roughness of the resting cells and degree of fluorescence around the mitotics. We were told mixed patterns should be rare, but we are seeing them fairly commonly. I have attached 3 images at a 1:160 taken on our Helios HTC using Aesku kits. We reported this as mixed homogenous speckled, but our lab is divided on if it could be DFS.
|
|
|
AC- |
What is the difference in using Hep2 cells cultures compared to monkey liver cells cultures....for what diagnostics are the monkey liver cells cultures better than Hep2 cells cultures... |
|
|
AC- |
Dear ICAP team and colleagues,
I was hoping to get your thoughts on this pattern, which I have noted in two children, both presenting with neurological conditions. Other neurological antibody work-up was negative. I understand that Cajal body is noted in neurons. There are clear few nuclear dots seen in the patients, with what we have also chosen to call as a speckled pattern also. Both dilute up to 640, using EUROimmun HEp-2 slides.
My questions are:
1. How would you label/define this pattern?
2. Have you seen associations with neurological conditions with AC-7?
Many thanks for your time and expertise.
I have attached 2 pictures at our start dilution of 1:160 for both patients. |
|
|
AC- |
Buen dûÙa a todos, espero se encuentren con bien, vengo a exponer un caso atûÙpico y creo que aun no existe clasificaciû°n para este AC-4, planeo reportarlo como AC-X, pero podrûÙa ser una subclasificaciû°n de AC-4 o bien, podrûÙa estar pasando por alto informaciû°n que desconozco.
Contexto:
Paciente femenino de 39 aûÝos
Perfil ENA:
Scl-70: POSITIVO
Jo-1: Zona gris
Nota: Se evalû¤a por duplicado el PERFIL ENA
Anticuerpos anti celulares(ANA): MARCA: Euroimmun, Sustrato: HEp-20-10/HûÙgado de mono,
Se hacen varias diluciones: desde 1:40 para rastreo de AC-20 por la posible presencia de JO-1, siendo este NEGATIVO en las celulas HEp-20-10 pero en ZONA GRIS por inmunoblot.
Se hacen diluciones segû¤n proveedor(Euroimmun): 1:100, 1:1000 y 1:10 000
Dando un patrû°n: AC-4 con marcada fluorescencia en la periferia de la placa metafûÀsica, pero placa metafûÀsica: NEGATIVA.
Citoplasma: granular fino denso tipo AC-19
cûˋlulas en anafase y telofase con fluorescencia en cromatina: NEGATIVA.
Se hace bû¤squeda de regiones NOR con empleando varias diluciones y planos focales siendo: NEGATIVAS
De modo que la tinciû°n no cumple con los criterios de un patrû°n AC-29 Topoisomerasa I(SCL-70) a pesar de estar positivo por inmunoblot(marca euroimmun)
Encontrûˋ artûÙculos donde algunas pacientes con miopatûÙas generaban un AC-4 pleomû°rfico con anafases y telofases: POSITIVAS, metafase NEGATIVA pero con marcada fluorescencia en la periferia de la placa metafûÀsica como en mi caso.
(AC-X: Characteristic Antinuclear Antibody Patterns of Two Anti-Mi-2 Autoantibody-Positive Dermatomyositis Patients-A Case Report, DOI: 10.3389/fimmu.2022.857030)
Adjunto imûÀgenes de IFI e Inmunoblot.
y me agradarûÙa saber su recomendaciû°n para el reporte de este tipo de patrones
Sin mas por el momento, quedo pendiente de su respuesta y les enviû° un cordial saludos desde Puebla, Mûˋxico.
ATTE: QFB Henry Guerrero Mtrz.
|
|
|
AC- |
Hello Drs. Chan and Andrade,
I hope this message finds you well. My name is Danielle Cervasio and I am on the Scientific Affairs team at EUROIMMUN US. We are creating some educational materials related to the new 2024 ICAP publication. For this, I would like to use some images off the ICAP website. Do we need any special permissions for this, or is citing "anapatterns.org" sufficient? Please let me know your thoughts, I look forward to hearing from you.
Kind regards,
Danielle Cervasio |
|
|
AC- |
We are seeing Hep 20-10 cells with a positive condense chromosomes. Positive metaphase plate but confirmatory tests for AC1 or AC2 are negative.
We are not sure how to report this?
|
|
|
AC- |
Admirado equipo del ICAP, reciban un cordial saludo. Mi pregunta: Cuando realizo un cambio de sustrato (marca) y observo una fluorescencia de un tûÙtulo en lo que antes era negativo, ô¢quûˋ herramientas puedo usar para estandarizar que ahora esta nueva intensidad de fluorescencia es mi nuevo negativo? adjunto fotos de mi û¤ltimo montaje. Gracias. |
|
|
AC- |
Cuantas lecturas de patrones estan permitidos para un analista |
|
|
AC- |
When can we introduce the AC-30 pattern in reports since it is not yet listed on the online page?
I fully agree with this classification, I think it was even necessary, as in my daily laboratory practice I frequently observe this pattern and never knew exactly how to report it according to ICAP.
I described it as fine granular (AC-4) with a positive metaphase plate or marked according to the intensity of the fluorescence on it.
What reflex tests should we adopt for AC-30?
Should we report AC-30 if anti-DFS70 is negative and AC-2 if DFS70 is positive?ã |
|
|
AC- |
Resultados de ANA (homogûˋneo 1:1280) y DNA (pos 1:160) en el aûÝo 2024, actualmente se observa un resultado de ANA (negativo;dil 1:80) DNA(pos 1:80). es posible, en los ultimos meses he observado pacientes con diagnû°stico de lupus con anti-dsDNA positivo y ANA Hep-2 negativo |
|
|
AC- |
Dear ICAP Team,
upon the upload of the ANA Patterns classification tree, as HEp-2 manufacture, we would like to share this news in our blog:
https://www.medipan.de/de/news/
Would it be allowed to use the image of the classification tree in our post?
Best regards,
Dr. Stefano Frasca
Medipan & GA Generic Assays |
|
|
AC- |
I am investigating the clinical significance and potential comorbidity associated with rare ANA patterns, with a particular focus on the co-occurrence of AC-25 and AC-27 patterns. Both patterns have been documented in association with SARDs as well as other connective tissue disorders, yet their combined presence remains poorly characterized.
Given that comorbidity of specific ANA patterns is uncommon, I am interested in determining whether the simultaneous presence of AC-25 and AC-27 confers greater clinical significance than either pattern alone. While individual studies and resources, suggest a low positive predictive value (PPV) for any single autoimmune disease, I am exploring whether their coexistence may influence disease risk, severity, or organ system involvement.
Additionally, as both AC-25 and AC-27 have been described in the context of malignancies, I seek to understand whether their co-occurrence is associated with an increased oncological risk or a paraneoplastic phenomenon.
Specifically, I would like to examine:
- Does the concurrent presence of AC-25 and AC-27 enhance diagnostic specificity for any particular autoimmune or systemic disorder?
- Could the co-expression of these ANA patterns serve as a marker of subclinical immune dysregulation or a predisposition to developing SARDs or any other conditions?
- Which organ systems or pathological processes are most likely to be implicated in individuals with both patterns present?
-Is there any evidence supporting a mechanistic link between these autoantibodies and oncogenesis, particularly in malignancies known to have autoimmune involvement especially in regards to carcinoma and paraneoplastic syndrome?
I would greatly appreciate any insights or references that might clarify the clinical implications of these rare ANA patterns when they coexist. Please feel free to share any additional insights or direct me to any relevant resources that may further clarify this topic.
Thank you for your time.
|
|
|
AC- |
How do we interpret the different intensities of ANA, when there can be so many interobserver/microscopic/Filter/ Camera software variations?
|
|
|
AC- |
I found it difficult to interpret this picture Can you help me? Thank you |
|
|
AC- |
I found it difficult to interpret this picture Can you help me? Thank you |
|
|
AC- |
I found it difficult to interpret this picture Can you help me? Thank you |
|
|
AC- |
I found it difficult to interpret this picture Can you help me? Thank you |
|
|
AC- |
ENDOMYSIUM NEG ? |
|
|
AC- |
Buenos dûÙas, cû°mo puedo diferenciar el AC-2 del AC-30, en interfase veo los nû¤cleos con patrû°n moteado fino denso iguales pero en divisiû°n no estoy segura, unos estûÀn moteados, en otros como lisa? gracias |
|
|
AC- |
Hello
I want to ask about new course. I got the introduction course from ICAP. Now I hope to develop my self in autoimmune diagnosis. |
|
|
AC- |
Reporting of AC-26 vs AC-4 and AC-25. In my lab there is a dispute on how to report on patients with speckled nuclear staining and staining of the spindle fibers. Our most experienced colleague reports those patients as a combination of AC-4 and AC-25, only opting for AC-26 with patients that have almost homogenous staining of the nucleus. Shouldnãt all these patients be reported with AC-26? Is AC-25 not meant to be only for patients with isolated staining of the spindle apparatus? |
|
|
AC- |
GOOD AFTERNOON, HOW CAN I DIFFERENTIATE THE AC-2 PATTERN FROM THE AC-30 PATTERN? WHAT WOULD BE THE MORPHOLOGICAL CHARACTERISTICS OF THE INTERPHASE AND THE CHROMATIN OF EACH ONE AND WHAT IS THE MAIN DIFFERENTIATION? |
|
|
AC- |
YOUR INTERPRETATION LEASE |
|
|
AC- |
YOUR INTERPRETATION PLEASE |
|
|
AC- |
Boa noite., relativamente aos novos Padrûçes AC-30 e AC-31 como se apresentam os nû¤cleos no tecido ( fûÙgado de macaco)?
Por exemplo, no padrûÈo AC-30 os nû¤cleos no fûÙgado, apresentam fluorescûˆncia como no padrûÈo Homogûˋneo ?
E no AC-31 , comportam- se como no AC-5?
Muito obrigada, pela atenûÏûÈo dispensada. |
|
|
AC- |
With the new patterns AC- 30 and AC-31, how is the reaction in the hepatocyte nuclei, on tissue sections of primate liver ? Is it positive like AC-1 or negative like AC-2? |
|
|
AC- |
As a clinician, I would love to see an extra column that says what antibodies may be associated with the pattern and what conditions. As these patterns are increasing being reported, it would be good to have updated information about these , thanks! |
|
|
AC- |
Hay casos de ADN dudosos en improntas de Crithidia Luciliae, sobre todo en patrones de ANA citoplasmatico granular . ô¢quûˋ interferencias o quûˋ patologûÙas pueden hacer que las C. Luciliae algunas se vean negativas, otras positivas o dûˋbilmente positivas, mezcladas en un mismo suero de paciente? |
|
|
AC- |
Hello, my name is Khwankamon, a laboratory techniqcian in Siriraj Hospital, Thailand.
We now facing an issue that we often found some patient with anti-Sm or anti-nRNP/Sm positive in Line Immunoassay, but the the ANA result is negative or positive with pattern that is not associated with the LIA result.
We suspected that this might be a false positive result from LIA or not? We are unsure if which one is more reliable?
Hopefully, we can help answer my question. We want to hear idea on this issue. |
|
|
AC- |
Dear ICAP Coordinators,
I hope this message finds you well.
I am a rheumatologist working at a governmental healthcare facility. Historically, our laboratory has employed a two-step process for antinuclear antibody (ANA) testing: an initial screening using ANA ELISA (via CLIA technique), followed by confirmation with manual ANA indirect immunofluorescence (IF) testing if the ELISA screening was positive.
Recently, our only immunologist has left the institution, and consequently, the manual ANA IF testing will no longer be available. In light of this change, I seek your expert guidance on the following:
1- Do you recommend relying solely on the ANA ELISA (CLIA) test as a screening tool in the absence of confirmatory manual ANA IF testing?
2- Would you advise investing in a digital ANA IF reader to replace manual IF testing? If so, could you kindly recommend manufacturers or specific models known for accuracy, reliability, and ease of use?
Your insights will greatly assist us in maintaining high-quality diagnostic standards for our patients.
Thank you very much for your time and support. I look forward to your valuable recommendations.
Kind Regards,
Dr. Majeed Haider |
|
|
AC- |
Hello, this IFA of my patient in which has no symptoms of lupus but lab insists it is positive speckle with titre 1:2500 and other said it is just 1:80, so plz can you give your opinion |
|
|
AC- |
IS NUCLEAR QUASIHOMOGENOUS A PATTERN TO BE REPORTED? |
|
|
AC- |
ô¢CuûÀl es la variaciû°n mûÀxima permitida entre operadores en la lectura de una misma muestra de ANA por IFI? |
|
|
AC- |
We would like to seek the help of the ICAP coordinates to advice us based on your experience the classification of the following ANA images.
The three images are serum from a patient tested on Euroimmun Hep-20-10 slides, initial screening at dilution of 1:160 followed by dilution at 1:320 and 1:640.
Would it be right to say this is a case of mixed patterns? Perhaps AC4 + AC7, though the AC7 do not look particularly convincing. |
|
|
AC- |
We would like to seek the advice of the ICAP coordinates to help identify this particular staining pattern we observed or advise if it is an artifact of the test procedure or sample.
The patient serum was tested on Euroimmun Hep20-10 slides at initial screening dilution of 1:160, followed by 1:320 and 1:640. We observed a singular bright stain in most interphase cells at 1:160, which is still vague visible at 1:320 (<1+ intensity). |
|
|
AC- |
Hello,
I have seen the new classification of ANA patterns and have a question regarding AC-31. From what I understand, AC-31 is strongly associated with anti-Ro60 antibodies.
In our laboratory, we use HEp-2000 cells (instead of standard HEp-2), which have the advantage of directly discriminating Ro60 by producing a characteristic pattern under the microscope. Therefore, for us, AC-31 seems both feasible and straightforward to identify with our current methodology.
Could you please confirm or clarify whether this reasoning is correct?
Kind regards,
Gû¥lsen Mutluoglu
Clinical Biologist, Belgium |
|